CASE STUDY
At Kupono Solutions, our reviews go beyond coding alone
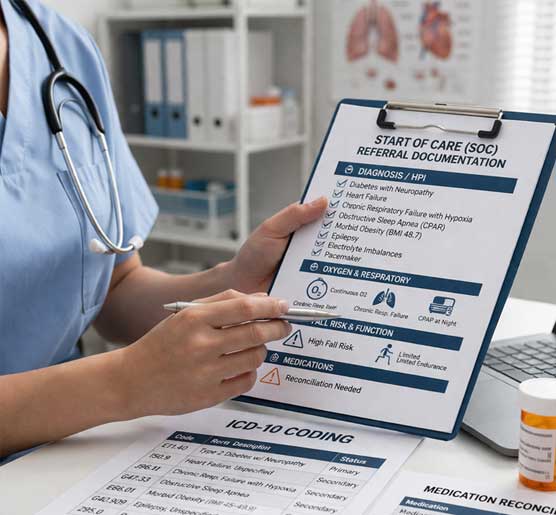
We evaluate how ICD-10 coding, OASIS, and the Plan of Care work together — identifying gaps, inconsistencies, and areas that require alignment.
Each case below reflects real scenarios across Start of Care, Resumption of Care, Recertification and Discharge. These examples highlight the types of findings that can occur throughout the home health episode and the level of detail applied during our RN-led reviews.